VI.1. Phototherapy and Radiation Protection
85% of all sensory perceptions are optical in origin but optical radiation is not only involved in the process of human vision, it has many other biological effects as well.
The photobiological effects of optical radiation, especially in the ultraviolet and blue (400 to 500nm) spectral regions, can be therapeutic. For example, it is used in phototherapy to treat a variety of skin diseases and in postnatal treatment of Hyperbilirubinemia. For proper dosimetry, irradiance (W/m2) and irradiance dose (J/m2) delivered by UV sources in phototherapy processes need to be monitored and controlled through accurate measurements. These measurements are typically performed with a spectrally and spatially qualified UV-A, UV-B and UV-B311 radiometer.
However, optical radiation also poses a potential health hazard for both human skin and eyes. For example, overexposure to ultraviolet and blue 'light' can cause common sunburn, photokeratitis (welder's eye) and burning of the retina or cornea.
Because of the dramatic increase in global UV radiation and the cumulative nature of the harmful effects, the additional risk of UV exposure by artificial sources is a concern.
The efficiency of protective devices like sun creams, UV blocking fabrics and sunglasses are the subjects of study.
Photobiologists, industrial hygienists, health and safety officers measure UV irradiance (W/m2) and irradiance dose (J/m2) of solar and artificial light sources in the lab, field and in the work place in order to study both the harmful and helpful effects of light and establish safe guidelines for its use. It is important to note that UV levels and subject exposure times typically vary so datalogging over some time period is commonly employed.
Because Gigahertz-Optik is actively involved in the "Thematic Network for Ultraviolet Measurements" funded by the Standards, Measurements and Testing program of the Commission of the European Communities, the detector and instrument designs are at the highest available level. The CIE, Commission Internationale de l'Eclairage, is reviewing many of the concepts put forth by the European Commission in an effort to internationally standardize the evaluation of UV radiometric measurement instrumentation much like the way photometric instruments are characterized now.
Incoherent Optical Radiation Protection
Even though there are many wide ranging and highly positive effects of light there are also negative effects to consider. Naturally occurring optical radiation, especially in the UV range of the solar spectrum, poses a potential health risk to outdoor workers and others who spend a significant amount of time outdoors. The most serious long-term consequence of UV exposure is the formation of malignant melanoma of the skin, a dangerous type of cancer. In the US, skin cancer is the most frequently contracted type of cancer, and since the 1970s, the incidence rates of malignant melanoma have more then doubled. As a similar development can be found for other countries, national and supranational networks of solar UV detectors have been established recently to monitor solar UV levels and the World Meteorological Organization is currently preparing guidelines for their characterization, calibration and maintenance.
Fig.VI.1. Incidence rates of malignant melanoma in the US since 1973.
In simple terms, incoherent optical radiation is optical radiation in the range of wavelengths between 100 nm and 1 mm, other than that emitted by lasers. The effect of incoherent optical radiation on the skin and the eye is being afforded increasing attention. The reasons for this are to be found in the rising exposure to radiation from sunlight, particularly in the UV range, and the growing use of high powered lamps in radiation therapy, radiation cosmetics, UV radiation curing, UV sterilization, vehicle headlamps, lighting equipment, etc. The high proportions of UV and blue light in the emission spectra of these lamps can, in addition to their desired effects, also result in radiation damage through both direct and indirect contact if the maximum permitted exposure levels are exceeded.
The shallow depth of penetration of optical radiation restricts the health hazards primarily to the eye and skin.
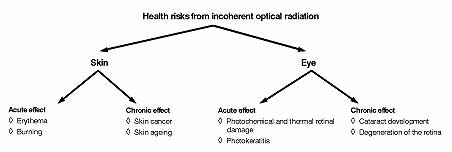
Fig.VI.2. Optical Radiation Health Risks
Relevant Radiation Quantities
When evaluating the harm that might be caused by incoherent optical radiation, it is the effective radiance (or the time integral of the radiance) that is critical for the retina, whereas for the skin, cornea and lens of the eye the critical quantity is the effective irradiance (or the exposure, also known as the dose) that can, for instance, arise at a workplace or in some other location where time is spent.
Photobiologically effective radiance
(W/(m2 sr))
with Le?(?): spectral radiance of the radiation sources
Photobiologically effective irradiance
(W/m2)
with Ee?(?): spectral irradiance of the radiation sources
Photobiologically effective exposure
(dose, J/m2)
with s(?)biol,rel stands for the relevant spectral response functions of the skin and eye.
If exposure limits are given in guidelines as effective radiance, Limit, or as effective irradiance, Elimit, then the following conditions should be maintained:
Ebiol = Elimit or Lbiol = Llimit
If the exposure vaues are given as the time integral of the radiance Li or as the exposure (dose), H, then the maximum permissible exposure duration, t, can be calculated:
t = Li / Lbiol or t = H / Ebiol
ACGIH / ICNIRP Spectral Weighting Functions for Assessing UV Radiation Hazards
The spectral weighting function for the acutely harmful effects of UV radiation, was developed by the American Conference of Governmental Industrial Hygienists (ACGIH) and the International Commission on Non-Ionising Radiation Protection (ICNIRP)
If one examines the spectral curve describing this function, it is seen that the spectral effectiveness in the UV-C and UV-B ranges is very high, and that it falls drastically in the UV-A range. The reason for this is that the function is derived from the functions relating the radiation to erythema (skin reddening) and photokeratoconjunctivitis (corneal inflammation). The range of wavelengths from 315 to 400 nm (UV-A) corresponds to a rectangle function representing total UV-A. Threshold Limit Values given for the maximum permissible exposure of the skin define the range of wavelengths as 200 (180) to 400 nm in reference to the ACGIH-ICNIRP function. The limits of maximum permissible exposure for the eye in the range 200 (180) to 400 nm and 315 to 400 nm (UV-A) are defined separately. By definition ACGIH-ICNIRP UV-C/B is measured in effective irradiance according to the spectrally weighted function and the UV-A level is assessed by measurement of the total UV-A irradiance (no spectral weighting function) for UV-A rich sources.
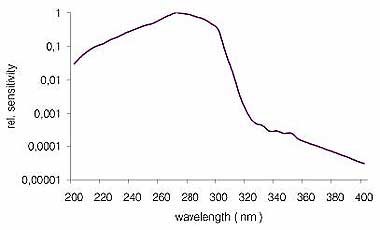
Fig. VI.3. ACGIH Spectral Function
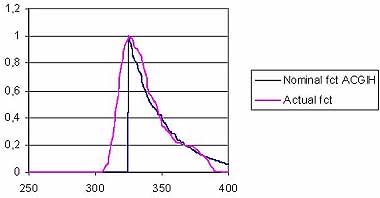
Fig. VI.4. ACGIH/ICNIRP UV-A Function
Blue-Light Hazard and Retinal Thermal Hazard Functions for Photochemical and Thermal Risks to the Retina
Blue Light Hazard (BLH)
If optical radiation with wavelengths between 380 and 1400 nm of sufficient intensity reaches the retina it can cause photochemical and thermal injury. Radiation in the "blue" part of the spectrum from 380 to 700 nm (effectively 380 to 550 nm) triggers photochemical reactions, if the photon energy in the radiation is high enough, converting chemically unstable molecules into one or more other molecule types. The spectral curve of the blue light hazard response function is shown in the following diagram. ICNIRP 1997 gives the following limits for the effective radiance of the BLH function:
LBLH * t = 100 J*cm-2 * sr-1 for t = 10.000s
LBLH = 10 mW * cm-2 * sr-1 for t > 10.000s
LBLH = effective radiance
t =duration of exposure
The blue light hazard function generally applies to exposure periods of more than 10 s. For shorter exposure times, the thermal retinal injury function applies.
Thermal Injury to the Eye -(RTH - Retina Thermal Hazard)
If the retina is exposed during short periods to high radiation intensities, a temperature rise to 45°C leads to hyperthermia, to 60°C causes coagulation, and to over 100°C results in vaporization. Removing the heat depends for the most part on the capacity of the irradiated zone to transfer heat, and thus on the size of the image of the radiation source on the retina. The diagram above illustrates the spectral response function for thermal damage to the retina according to ICNIRP.
In the spectral range between 380 and 500 nm, the effect of the RTH function is larger than the BLH function by a factor of 10. Whereas the latter rapidly falls to zero above 500 nm, the thermal function continues on to 1400 nm. Since no industrially useable radiation sensors with spectral sensitivity from 380 to 1400 nm exist, an acceptable simulated match using silicon photodiodes is in use. In this context it is quite adequate to measure the range up to 1200 nm, since various light sources exhibit no more than 4% difference in the integrated totals to 1200 nm and to 1400 nm. This statement is also confirmed by ICNIRP in their working paper /1/.
For radiation sources whose emissions lie primarily in the near infrared range (IR-A) between 780 and 1400 nm, and that generate a visual luminance of less than 10 cd/m2, the visual stimulus is so weak that the aversion reflex is not activated. In such applications the measurement of radiance must, according to ICNIRP, take place exclusively in the IR-A region.
L(?): spectral radiance of the radiation source being measured, RTH(?) : Retina Thermal Hazard Function,a
= apparent radiation source.
Limits are also prescribed for the RTH function. Thus, for the case where
10μ = t = 10s
Lhaz = 50/( a*t 0,25) (kW*m-2*sr-1 )
Lhaz = effective radiance for the RTH function,
a = size of the light source expressed in radians
For t < 10 μs the limit must not be any greater than Lhaz for t= 10 μs. For t > 10 μs the limit must not be any greater than Lhaz for t= 10 s.
Metrological Considerations
Radiance is the quantity relevant to the evaluation of BLH and RTH hazards. The latest draft standards (IEC 825-1, November 1998), and ICNIRP (printed in Health Physics 1999) express views as to the angle of the measurement field of radiance meters. The applicable figures related to exposure durations are:
t
<10s an a of 1.7mrad 1) ;
t=10s...100s an a of 11mrad 2)
t= 100s...10000s an a of 1.1*t 0,5 2),
t> 10000s an a of 100mrad 2)
1) Dominance of thermal damage to the retina
2) Dominance of blue light hazard
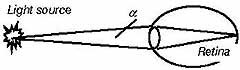
Fig. VI.5. Light Source - Subtended Angle — Retina
For RTH IR-A evaluation ANSI/IESNA RP-27.1-96 recommends a field of view of 11 mrad, and of 100 mrad for very large radiation sources.
/1/ ICNIRP: Guidelines of limits of exposure to broad-band incoherent optical Radiation (0,38μm to 3 μm) (September 1997)(0,38μm to 3 μm) (September 1997)
Fig. VI.6. Retinal Thermal & Blue Light Hazard Spectral Functions
UV-Erythema
The typical symptom of UV erythema is acute skin inflammation caused by UV radiation (sunburn). It used to be thought that erythema was only caused by radiation components in the UV-B range of wavelengths. Present opinion is that UV-A plays a part in causing erythema because there is so much more of it present. Medical investigations have shown that intensive exposure to UV in leisure time and at work increases the risk of skin cancer. Children in particular should be protected from strong UV radiation, as the skin stores the information about the UV dose received in the first years of life, and this can be an important factor in the development of skin tumors in later years.
Sunburn occurs in fair-skinned people (skin type 2) with a UV dose of as little as 250 J/m². Our table (following F. Greiter: Sonne und Gesundheit, (Sun and Health), published by Gustav Fischer Verlag 1984) lists the various exposure duration's for minimal skin reddening for different skin types.
Fig. VI.7. Erythemal Spectral Function
Skin type |
Description |
Identification |
Reaction to the sun |
|
Exposure duration ( min ) |
I |
Skin: noticeably light; Freckles: strong; Hair: reddish; Eyes: blue, rarely brown; Nipples: very pale |
Celtic type (2 percent) |
Only very painful |
No reddeningwhite after 1 to two days, skin peels |
5 to 10 |
II |
Skin: somewhat darker than I |
Light skinned European (12 percent) |
Only very painful |
HardlySkin peels |
10 to 20 |
III |
Skin: light to light brown, fresh |
Dark skinned European (78 percent) |
Moderate |
Average |
20 to 30 |
IV |
Skin: light brown, olive; Freckles: none; Hair: dark brown; Eyes: dark; Nipples: dark |
Mediterranean type (8 percent) |
Hardly |
Fast and deep |
40 |
Table VI.1. Skin Type Categories
Phototherapy
UV-A, UV-B and UV-B311 Phototherapy
UV is widely used by dermatologists in the treatment of certain skin diseases like Psoriasis and Vitiligo. Whole body exposure booths and hand and foot units employing light sources which emit broadband UV-A, UV-B, narrowband 311nm UVB and combinations of UV-A and UV-B are used to irradiate the patient.
In PUVA phototherapy, also called photochemotherapy, UV-A is applied in combination with a photosensitizing agent which is taken in pill form or applied topically to the skin. This medication called psoralen, giving rise to the acronym PUVA, makes the skin more sensitive and responsive to the UV-A (315-400nm) wavelengths.
Due to the risks of premature skin ageing and skin cancer from prolonged exposures, also with consideration to skin type, PUVA is only recommended for moderate to severe cases of Psoriasis. As a side note, psoralen is also being used as a photosensitizer in UV sterilization of blood.
UV-B broadband treatment is normally administered without a photosensitizing agent. It is considered safer than UV-A for wavelengths between approx. 290 to 315 nm, since it does not penetrate as deeply into the skin and is more energetic allowing shorter overall exposure times. However, it is generally accepted that wavelengths below 290 nm produce more erythema which can actually inhibit the therapeutic effects of the longer wavelengths.
As a result, narrowband UV-B sources emitting at predominantly 311-312 nm, have been developed. They emit right in the wavelength zone of most effectiveness while producing less erythemal interference than broadband UV-B sources.
This is generally known as a TL-01 source. A TL-12 UV-B source with a slightly wider band of emittance between 280-350 nm, peaking at about 305 nm is also in use. For more information contact the National Psoriasis Foundation and the American and European Academies of Dermatology.
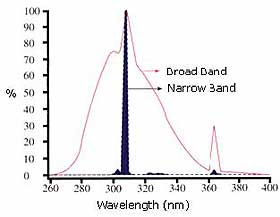
Fig. VI.8. Narrowband 311nm & Broadband UV-B Source Spectra
Dose, used here as irradiance accumulated over time, is normally measured in phototherapy applications.
joules/cm² = watts/cm² x seconds
(dose/energy) = irradiance x time
In the research & development stage or field service, direct irradiance may be monitored to discern any variation in output through lamp or delivery system degradation but most of today's phototherapy equipment is equipped with sensors and electronics which allow delivery of pre-selected doses of UV.
Third party checks of these internal dosimeters by qualified UV radiometers is recommended to ensure proper dosimetry and safety.
Bilirubin Phototherapy
Newborn jaundice or neonatal hyperbilirubinaemia, a yellowish appearance of the skin and whites of the eyes, is present to some degree in almost all newborn infants. This is caused by an elevated level of bilirubin molecule in the blood which results from immaturity of the liver function combined with the destruction of red blood cells present. When these levels are very high, one method of clearing the jaundice is by exposing the newborn to light in the blue spectral region between 400 to 550 nm. The light interacts with the bilirubin, converts it to a substance excreted back into the bloodstream which can then be excreted in the feces. The newborn is placed nude in a 'bilibed' or protected isolette and exposed to fluorescent lights designed or filtered to emit in the blue spectrum. A recent development is the 'biliblanket' that delivers blue light through fiber optics and can be wrapped around the infant. Radiometric measurements of bililights are important in order to ensure proper dosimetry.
Efforts to standardize an action spectral function and measurement procedures for bilirubin are in process. Due to early work in this field, the units of microwatts/cm²/nm were wrongly adopted for radiometric measurement of bililights. To be technically correct the units of watts/cm² should apply.
Fig. VI.9. Bilirubin Spectral Function
Tutorials

Copyright © 2008 - 2025 Gigahertz-Optik, Inc. All Rights Reserved